Thyroid Med Cessation Risks
Abruptly halting thyroid hormone replacement therapy—such as levothyroxine, liothyronine, or natural desiccated thyroid (NDT)—rapidly depletes the body’s circulating hormone pools, triggering cellular metabolic shock. When exogenous thyroid hormones are suddenly withdrawn, target tissues lose their primary regulator of energy production, leading directly to systemic hypothermia, cardiovascular strain, severe lipid disruptions, and cognitive deterioration. For patients utilizing anti-thyroid medications like methimazole or propylthiouracil (PTU) for hyperthyroidism, abrupt cessation causes an uninhibited rebound of thyroid hormone synthesis, putting the patient at immediate risk of a high-mortality thyrotoxic crisis.
If you have missed multiple doses, are experiencing uncomfortable side effects, or are considering adjusting your thyroid regimen, you must navigate these changes under strict clinical observation. Attempting to cease therapy without a systematic taper and active serum monitoring can result in acute, life-threatening medical emergencies.
Cell Metabolism Deficit Dynamics
Exogenous thyroid hormones exert a profound influence on almost every cell in the human body. To understand what happens when these medications are stopped, one must look at the transcriptional control thyroid hormones have on cellular DNA.
Pharmacokinetics of Levothyroxine
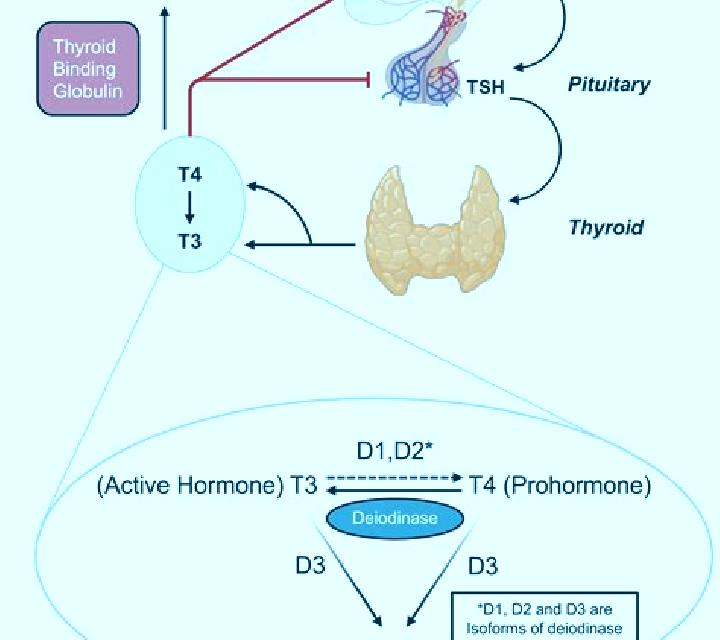
Levothyroxine (synthetic $T_4$) serves as a prohormone reservoir, binding heavily to thyroxine-binding globulin (TBG), transthyretin, and albumin in the bloodstream. It features a long elimination half-life of approximately seven days in euthyroid individuals, which can extend up to ten days in hypothyroid patients. When you stop taking levothyroxine, the clinical decline is slow and insidious.
For the first three to five days, you may feel completely normal because the circulating pool of bound $T_4$ slowly releases free hormones into the tissue. However, as these tissue stores systematically deplete over a three- to four-week period, the intracellular conversion of $T_4$ to the active $T_3$ hormone drops significantly. This structural delay often misleads patients into believing they no longer need their medication, only to experience an intense physiological crash once serum levels fall below metabolic threshold limits.
| Hormone Type | Active Compounds | Plasma Half-Life | Storage Depletion Speed | Target Receptor Affinity |
|---|---|---|---|---|
| Levothyroxine (Synthroid) | Synthetic $T_4$ | 7 to 10 days | 4 to 6 weeks | Low (requires conversion to $T_3$) |
| Liothyronine (Cytomel) | Synthetic $T_3$ | 18 to 24 hours | 48 to 72 hours | High (direct nuclear binding) |
| Desiccated Thyroid (NDT) | USP $T_4$ and $T_3$ mix | Bi-phasic (combined) | Variegated (1 to 3 weeks) | High (due to direct $T_3$ content) |
Rapid Depletion of Liothyronine
In contrast to $T_4$, liothyronine (synthetic $T_3$) has a short half-life of less than 24 hours. Because it does not bind strongly to serum proteins, it interacts directly with nuclear thyroid hormone receptors. Abrupt withdrawal has immediate consequences. Within 48 hours of stopping $T_3$, intracellular transcription of vital metabolic enzymes stalls.
Without the bound $T_3$ ligand, thyroid hormone receptors bind to thyroid hormone response elements (TREs) on DNA along with co-repressor molecules, actively suppressing gene expression. This molecular shift leads to a rapid decline in cellular respiration, oxygen consumption, and adenosine triphosphate (ATP) production.
- Downregulation of mitochondrial activity: Deprivation of $T_3$ reduces the transcription of mitochondrial genes involved in oxidative phosphorylation, leading to a profound cellular energy deficit.
- Sodium-Potassium pump failure: Synthesis of the $Na^+/K^+$-ATPase pump declines, hindering basic electrochemical gradients across cellular membranes and causing cellular swelling and fluid imbalances.
- Mucopolysaccharide accumulation: The breakdown of glycosaminoglycans slows, causing these compounds to accumulate in the interstitial spaces of skin and visceral organs, which leads to general myxedematous edema.
- Hepatic clearance reduction: Low thyroid hormone levels in the liver decrease the expression of low-density lipoprotein (LDL) receptors, causing a rapid increase in circulating serum LDL cholesterol and triglycerides.
Acute Hypothyroid Crisis Danger
The most severe danger of stopping thyroid hormone replacement is myxedema coma. Despite its name, patients do not need to be in a flat-line coma to be diagnosed with this state; it represents the extreme end of decompensated hypothyroidism, characterized by multi-organ system failure driven by total metabolic collapse.
When thyroid medication is stopped, the body slowly loses its ability to generate heat and regulate blood volume. If the patient faces an additional physiological stressor—such as an infection, cold exposure, cardiovascular event, or administration of sedative medications—they can quickly transition from simple hypothyroidism to an acute, life-threatening emergency.
During myxedema coma, the thermoregulatory center in the hypothalamus fails without thyroid hormone activation. Body temperature can drop below 90°F (32.2°C). This severe hypothermia slows biochemical reactions, further depressing metabolic processes. Hypoventilation develops as the respiratory muscles weaken and the brainstem's sensitivity to hypoxia and hypercapnia decreases, leading to respiratory acidosis and cerebral hypoxia.
"Myxedema coma remains a highly lethal endocrine emergency, with mortality rates ranging from 30% to 50% even with aggressive intensive care support. Early replacement of intravenous thyroid hormones and stress-dose glucocorticoids is paramount to survival." — The American Thyroid Association (ATA) Clinical Guidelines Council
In addition, water clearance by the kidneys drops significantly due to impaired glomerular filtration rates and the inappropriate release of antidiuretic hormone (ADH). This causes severe dilutional hyponatremia, which lowers the seizure threshold and worsens cognitive decline, leading to stupor and eventually coma.
Cardiac and Cognitive Impacts
The heart and brain are highly sensitive to thyroid hormone levels. Sudden withdrawal of these hormones can cause rapid, serious problems in both organ systems.
Cardiovascular Dysfunction
Thyroid hormones directly control the expression of key proteins in cardiac cells, including the calcium pump ($SERCA2$) and beta-1 adrenergic receptors. By regulating these proteins, thyroid hormones help maintain normal heart contractions and heart rate. When you abruptly stop taking thyroid medication, these cellular pathways are disrupted, causing significant changes in cardiovascular function:
- Decreased Cardiac Output: Without thyroid hormones, the heart loses its pumping strength (inotropic capacity) and beats slower (chronotropic capacity), reducing overall cardiac output.
- Increased Systemic Vascular Resistance: Blood vessels lose their ability to relax, leading to stiffer arteries and an increase in diastolic blood pressure.
- Bradycardia and Arrhythmias: The heart rate slows, and the heart's electrical conduction system can become unstable, increasing the risk of heart block or QT-interval prolongation, which can lead to ventricular arrhythmias.
- Pericardial Effusion: Slow fluid accumulation within the pericardial sac can compress the heart and further reduce blood flow throughout the body.
Cognitive and Neuropsychiatric Decline
In the central nervous system, thyroid hormones regulate nerve signaling, myelination, and blood flow to the brain. When these hormones are withdrawn, synaptic transmission slows down, leading to a range of cognitive and psychiatric symptoms.
Initially, patients experience brain fog, memory lapses, and difficulty concentrating. Over time, this can progress to severe clinical depression that does not respond to standard antidepressant therapy. In some cases, patients may develop hypothyroid-induced psychosis, also known as "myxedema madness," which is characterized by paranoid delusions, visual and auditory hallucinations, and extreme confusion.
| Organ System | Euthyroid State | Abrupt Medication Cessation State | Long-term Clinical Consequence |
|---|---|---|---|
| Cardiovascular | Optimal stroke volume, active $SERCA2$ expression, normal systemic vascular resistance. | Bradycardia, reduced contractility, high peripheral resistance, diastolic hypertension. | Congestive heart failure, increased vascular stiffness, coronary ischemia. |
| Neurological | High-speed synaptic transmission, regulated serotonin synthesis, optimal memory function. | Cerebral hypoperfusion, slowed neural processing, synaptic signaling decay. | Severe depression, pseudodementia, myxedema madness, chronic cognitive deficits. |
| Renal | Normal glomerular filtration rate (GFR), balanced water clearance, stable sodium balance. | Decreased GFR, decreased renal blood flow, impaired free water excretion. | Hyponatremia, systemic fluid retention, drug toxicity from reduced renal clearance. |
| Gastrointestinal | Standard peristaltic waves, efficient nutrient absorption, regular bowel movements. | Intestinal hypomotility, slowed smooth muscle contraction, paralytic ileus. | Severe fecal impaction, toxic megacolon, systemic malabsorption. |
Anti-Thyroid Stoppage Risks
While stopping thyroid hormone replacement causes a severe metabolic drop, abruptly halting anti-thyroid medications (methimazole or propylthiouracil) for hyperthyroidism can trigger a highly dangerous hyper-metabolic state known as a thyroid storm.
Anti-thyroid medications work by blocking thyroid peroxidase (TPO), the enzyme responsible for binding iodine to thyroglobulin to create $T_4$ and $T_3$. When these medications are stopped suddenly, the iodine stored in the gland is rapidly processed, causing a massive release of active thyroid hormones into the bloodstream.
This sudden surge of thyroid hormones triggers hyper-responsiveness in beta-adrenergic receptors throughout the body, causing an intense adrenaline-like reaction. This can quickly escalate into a thyroid storm, a medical emergency characterized by extreme hyperthermia, rapid heart rates (often leading to atrial fibrillation), high-output heart failure, severe agitation, and delirium.
- Extreme Hyperpyrexia: Body temperatures can rapidly climb above 104°F (40°C), causing cell damage and dehydration.
- Tachyarrhythmias: Heart rates often exceed 140 beats per minute, which can trigger atrial fibrillation and lead to cardiovascular collapse.
- Congestive Heart Failure: The heart is forced to pump faster to meet increased metabolic demands, eventually exhausting the heart muscle and causing fluid to build up in the lungs (pulmonary edema).
- Hepatic Dysfunction: Severe hyperthyroidism can cause liver injury, leading to jaundice, abdominal pain, and liver failure.
- Central Nervous System Delirium: The patient may experience severe agitation, psychosis, seizures, or progress to a comatose state.
"Discontinuing thionamide therapy without medical supervision or an alternative treatment plan exposes hyperthyroid patients to unstable thyroid states and elevates the risk of a thyrotoxic crisis, which carries a 10% to 30% mortality rate." — British Thyroid Foundation Clinical Safety Bulletin
Bioavailability and Dosage Adaptation
In clinical settings, patients often stop their medications because they feel the therapy is not working, or because they are experiencing side effects from improper dosing or poor absorption. Understanding how to manage your dosage and ensure proper absorption is essential to keeping your thyroid levels stable without putting your health at risk.
Factors Affecting Hormone Absorption
Levothyroxine is primarily absorbed in the duodenum and jejunum. This process requires a highly acidic stomach environment and can be easily disrupted by food, beverages, and other medications. Many patients who believe their medication is ineffective are actually experiencing poor absorption due to common dietary or pharmaceutical conflicts:
- Administration timing: Taking levothyroxine with food or morning coffee can reduce its absorption by up to 30%. The medication should always be taken with a full glass of water on an empty stomach, either 60 minutes before breakfast or bedtime (at least 3 hours after your last meal).
- Interfering supplements: Calcium carbonate, ferrous sulfate (iron), magnesium, and aluminum-containing antacids bind directly to thyroid hormones in the digestive tract, preventing them from being absorbed. These supplements must be taken at least four hours apart from thyroid medications.
- Gastrointestinal conditions: Inflammatory bowel disease, celiac disease, H. pylori infections, and low stomach acid (often caused by proton pump inhibitors like omeprazole) can significantly impair medication absorption, leading to fluctuating thyroid levels.
| Interfering Compound | Mechanism of Action | Clinical Consequence | Recommended Management Strategy |
|---|---|---|---|
| Proton Pump Inhibitors | Increases gastric pH, reducing dissolution of thyroid tablets. | Incomplete drug absorption and elevated TSH levels. | Monitor TSH; take thyroid hormone on an empty stomach; adjust dose if PPI cannot be stopped. |
| Calcium & Iron Supplements | Binds to thyroid hormones in the digestive tract, forming unabsorbable complexes. | Significant drop in active hormone levels; return of hypothyroid symptoms. | Keep a strict minimum interval of 4 hours between dosing thyroid meds and these minerals. |
| Soy and High-Fiber Diet | Increases fecal excretion of thyroxine by binding to the hormone in the gut. | Unstable hormone levels; require higher doses of thyroid medication. | Maintain consistent daily fiber and soy intake, and adjust dosage accordingly. |
| Coffee / Espresso | Increases intestinal transit speed and interferes with drug dissolution. | Variable absorption; unexplained changes in TSH levels. | Avoid drink ingestion for at least 60 minutes after taking levothyroxine. |
Patient-Initiated Dosage Changes
When patients try to manage their own thyroid symptoms by adjusting their dosage or stopping their medication, they often trigger a cycle of unstable hormone levels. If you feel your dose is too high or too low, the solution is not to stop taking it, but to get a comprehensive thyroid panel (including TSH, Free $T_4$, and Free $T_3$) and work with your doctor to make precise, gradual adjustments.
Adjusting your medication based on how you feel can result in fluctuating between hyperthyroid and hypothyroid states. This places significant stress on your cardiovascular and endocrine systems, making it much more difficult to find a stable, effective dose.
"Self-adjusting thyroid medication based on subjective symptoms rather than objective, repeated laboratory assays disrupts the hypothalamic-pituitary-thyroid Axis feedback loop. This can cause severe cardiovascular stress and make clinical management highly complex." — Dr. Antonio Bianco, Former President of the American Thyroid Association
Clinical Patient Recovery Recommendations
If you have stopped taking your thyroid medication and want to restart safely, or if you need to adjust your current treatment plan, you should follow a structured clinical protocol:
- Assess Current Hormone Levels: Before restarting your medication, obtain a comprehensive thyroid panel (TSH, Free $T_4$, and Free $T_3$). This provides a clear baseline and helps your doctor determine the appropriate restarting dose, especially if you have been off your medication for several weeks.
- Determine the Restart Dose: Your doctor will evaluate your age, cardiovascular health, and how long you have been off your medication to find a safe starting dose. For younger patients with no cardiovascular risk, the full former dose can often be resumed. For elderly patients or those with existing heart conditions, the medication is typically restarted at a low dose (e.g., 12.5 mcg to 25 mcg of levothyroxine) and gradually increased to prevent cardiovascular side effects.
- Set a Consistent Dose Schedule: Consistency is key to successful thyroid therapy. Choose a daily schedule—either first thing in the morning or right before bed—that allows you to take your medication on an empty stomach, away from interfering food, caffeine, or supplements.
- Schedule Follow-Up Testing: It takes about six to eight weeks for thyroid levels to reach a stable state in the blood after starting or adjusting a dose of $T_4$. Schedule your follow-up blood tests during this window to ensure your dose is adjusted safely and accurately.
Restart Protocol:
[Stop Meds] ➔ [Order Thyroid Panel] ➔ [Determine Restart Dose] ➔ [Maintain Daily Bioavailability Protocol] ➔ [Re-test TSH in 6–8 Weeks]By following these clinical guidelines and working closely with your healthcare provider, you can safely restore and maintain your thyroid health, avoiding the serious risks of sudden medication changes.
Common Medical Inquiries Resolved
What happens to cellular energy if levothyroxine is stopped for one week?
When you stop taking levothyroxine for one week, your cellular energy levels begin to decline, though the change is often gradual. Because levothyroxine has a long half-life of about seven days, your body still has circulating thyroid hormones during this first week. However, as the levels of T4 and T3 inside your cells start to drop, the mitochondria begin to produce less ATP. You may start to experience early symptoms of this metabolic slowdown, such as mild fatigue, feeling cold, and a slower mental processing speed.
Can stopping hyperthyroid drugs abruptly trigger a cardiac event?
Yes. Abruptly stopping anti-thyroid medications like methimazole or propylthiouracil can trigger a sudden and severe increase in thyroid hormone levels. This surge causes your heart cells to become highly sensitive to adrenaline. This can lead to rapid heart rates, atrial fibrillation, and a high-output state that can trigger acute congestive heart failure or a myocardial infarction, especially in patients with existing heart conditions.
How long does it take for thyroid hormone levels to normalize after resuming treatment?
The time it takes for your thyroid levels to normalize depends on the type of medication you are taking. For levothyroxine ($T_4$), it typically takes six to eight weeks of daily, consistent use to build up stable hormone levels in your tissues and normalize your TSH. For liothyronine ($T_3$), serum levels rise much more quickly, often within a few days, though it still takes several weeks for your tissues to adjust and your overall symptoms to resolve.
Can stopping thyroid medication cause rapid weight gain that is permanent?
Stopping your thyroid medication can cause rapid weight gain, but this change is not permanent. The weight gain is primarily caused by two factors: a slower metabolic rate that leads to increased fat storage, and the accumulation of fluid and mucopolysaccharides in your body's tissues (myxedematous fluid retention). Once you resume your correct thyroid hormone dosage and restore normal metabolic function, your body will release the excess fluid, and your metabolic rate will return to normal, allowing you to manage your weight effectively.
Why does abruptly stopping thyroid pills make patients feel extremely cold?
Thyroid hormones directly control your basal metabolic rate and heat production by regulating the activity of the sodium-potassium pump ($Na^+/K^+$-ATPase) in your cells and stimulatig brown adipose tissue fat-burning pathways. When you stop taking your medication, your body's cellular heat production drops significantly. Your blood vessels also constrict in an effort to preserve core body heat, which reduces blood flow to your hands and feet, making you feel cold even in warm environments.
Is it safe to stop thyroid medication during pregnancy if TSH returns to normal?
No, it is highly dangerous to stop thyroid medication during pregnancy, even if your TSH levels appear normal. A normal TSH level indicates that your current medication dose is working correctly to support both your body and the developing fetus. Stopping your medication can lead to a rapid return of severe hypothyroidism, which increases the risk of serious complications, including miscarriage, preeclampsia, premature birth, and developmental or cognitive delays in the baby. Thyroid hormone requirements actually increase during pregnancy, meaning your dose may need to be adjusted upward, never stopped.